5258 - Cartilage, semilunar, dislocated, with frequent episodes of locking, pain, and effusion into the joint
DBQ: Link to Index of DBQ/Exams by Disability for DC 5258
Acronym: MMT
Definition
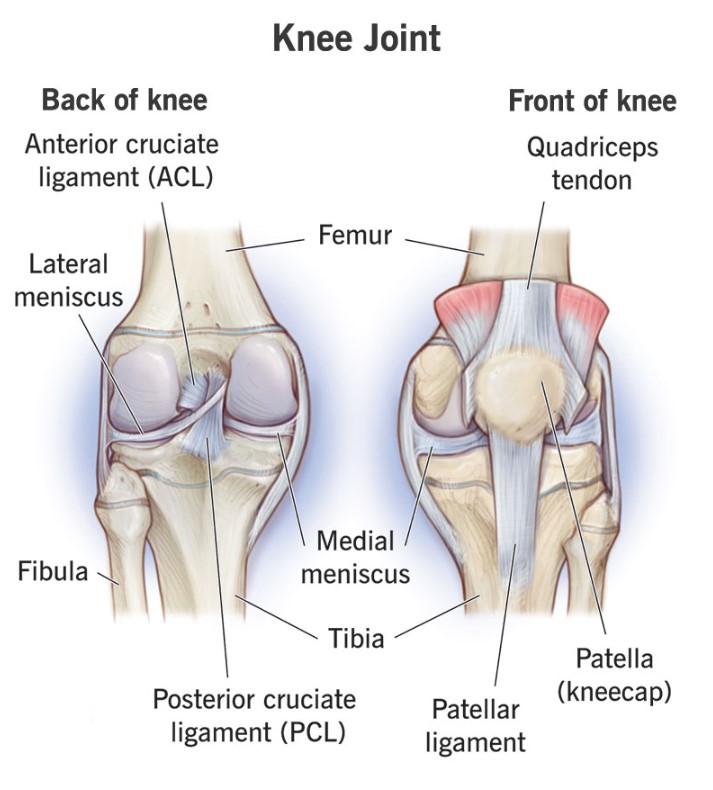
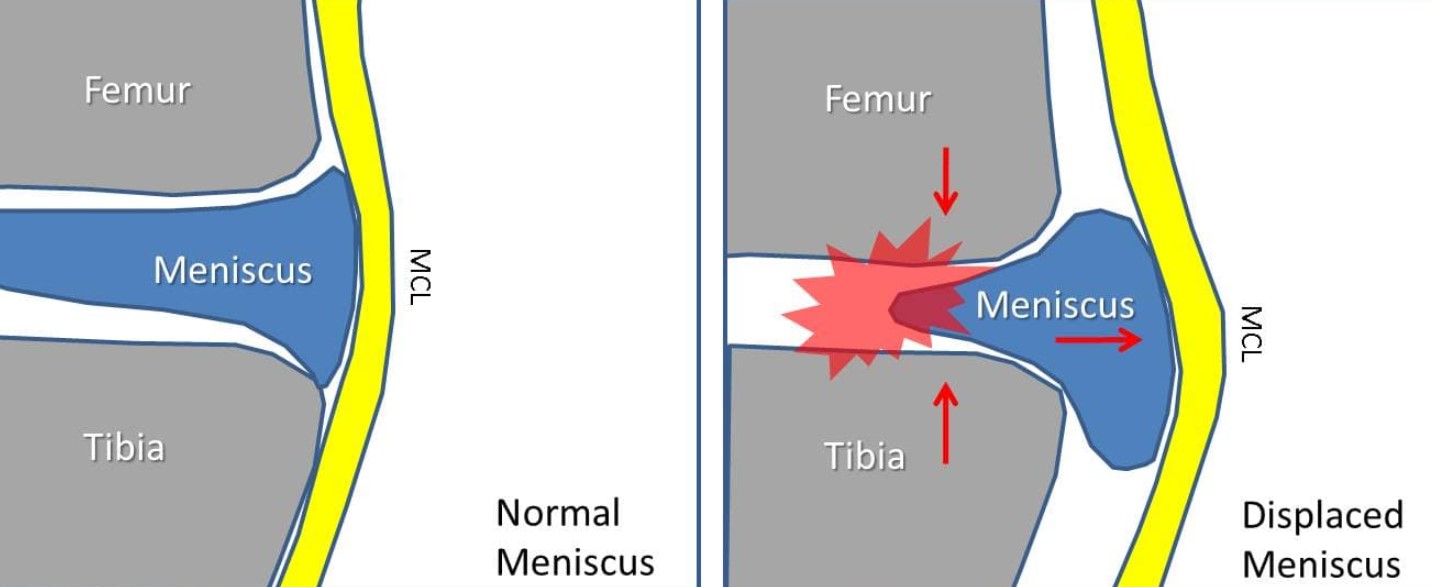
Semilunar cartilage refers to the medial crescent-like shape or lateral cartilages of the knee joint between the femur and the tibia. Dislocation refers to the displacement of any part from its normal position in a joint. Locking is the feeling of loss of extension secondary to a mechanical block; i.e. bucket handle tear meniscus. There may also be a sensation of buckling or giving way. Effusion is the escape of fluid into a part, in this case within a joint cavity. In this case, the involved joint is the knee.
{kind=link}
Etiology
Causes of dislocation may include: disease, such as arthritic degenerative diseases; trauma; congenital anomalies; cysts; infection; or metabolic disorders.
Signs & Symptoms
Manifestations presented may include: effusion or increased production of synovial fluid; pain; swelling; inflammation; popping sensation; locking; giving way sensation; instability; inability to bear weight; or catching sensation.
{kind=link}
Tests
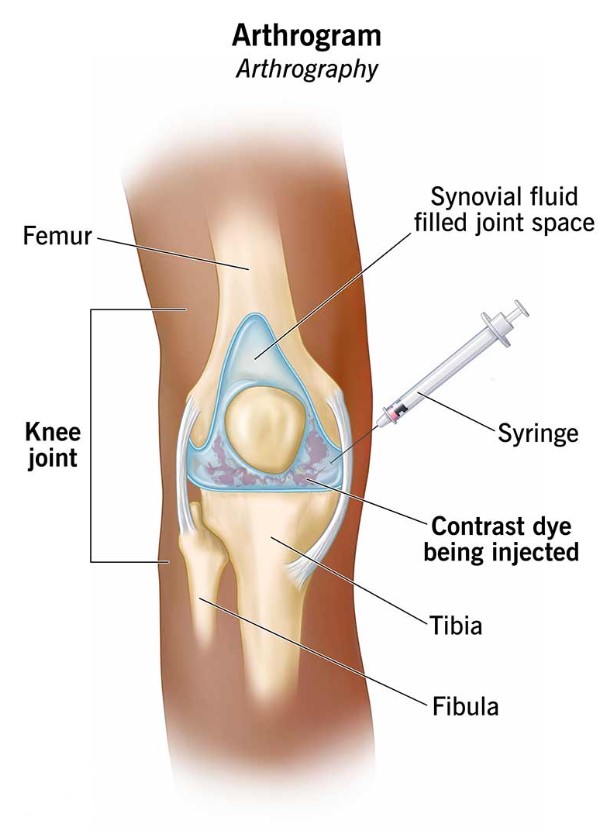
Tests which are carried out include: physical examination, and range of motion tests such as McMurrays sign. In addition, contrast arthrogram, magnetic resonance imaging (MRI), and arthroscopy may also be done to confirm a diagnosis. MRI is more sensitive for medial than lateral meniscal tears.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Early conservative treatment may include: immobilization; bracing; protective weight bearing; and exercises. Manipulation with traction may be attempted. For recurrent or persistent signs and symptoms, arthroscopic treatment may be necessary for repair. Before or after surgery, physical therapy appropriate to the type of injury may be required. Medication for pain or inflammation may be given.
{kind=link}
Residuals
The outcome may depend on the location of the tear and the amount of remaining healthy meniscus. With conservative treatment, the outcome is good. If the tear involved the vascularized portion of the cartilage, the potential for repair is also good. Mobility may be limited, and the development of osteoarthrosis or avascular necrosis is possible. Those patients refractory to non-operative treatment should be offered arthroscopy.
Special Considerations
-
The rating schedule for musculoskeletal was updated on February 7, 2021. Protection still does apply and should be considered with existing evaluations (38 CFR 3.951(a)).
-
DC 5258 was updated November 29, 2017, based on the holding in Lyles v. Shulkin, 29 Vet.App. 107 (2017). Prior to the Lyles holding, separate evaluations for meniscal disabilities under 38 CFR 4.71a, DC 5258 or DC 5259 and other knee evaluations under 38 CFR 4.71a, DC 5257, 5260, or DC 5261 were prohibited. This is not considered a liberalizing change.
-
The rating schedule for musculoskeletal was updated on February 7, 2021. Protection still applies and should be considered, under 38 CFR 3.951 and 38 CFR 3.957.
-
Evaluation of a knee disability under 38 CFR 4.71a, DC 5257, DC 5260, or 5261 does not, as a matter of law, preclude separate evaluation of a meniscal disability of the same knee under 38 CFR 4.71a, DC 5258 (dislocated semilunar cartilage), or 38 CFR 4.71a, DC 5259 (symptomatic removal of semilunar cartilage).
-
A meniscal disability may be rated separately under 38 CFR 4.71a, DC 5258/5259 apart from 38 CFR 4.71a, DC 5257 for manifestations of the knee disability other than recurrent subluxation and instability, and/or 38 CFR 4.71a, DC 5260/5261 if a manifestation of the meniscal disability did not result in an elevation of the disability evaluation warranted under 38 CFR 4.71a, DC 5260/5261 via application of 38 CFR 4.40 and 38 CFR 4.45 pursuant to DeLuca v. Brown, 8 Vet.App. 202 (1995).
-
A repaired meniscal tear (s/p partial meniscectomy) is not directly synonymous with either 38 CFR 4.71a, DC 5258 or 38 CFR 4.71a, DC 5259. Therefore, it is most appropriate to rate the disability analogous to whichever code most closely approximates the current symptoms.
-
Entitlement to a separate evaluation for the meniscal disability depends on whether the manifestations are utilized to assign an evaluation under a different DC. Evaluation of the same manifestation under multiple diagnoses is prohibited under 38 CFR 4.14. Thus, when all the symptoms of the meniscal disability are used to support elevation of an evaluation under 38 CFR 4.71a, DC 5260/5261 or assignment of an evaluation under 38 CFR 4.71a, DC 5257, a separate evaluation cannot be assigned under 38 CFR 4.71a, DC 5258/5259.
-
When considering applicability of 38 CFR 4.59 for meniscal disabilities, when only a meniscal disability is present, utilize the procedures at M21-1, Part V, Subpart iii, 1.A.1.m, and when multiple knee disabilities are present and the painful motion is attributable to a knee disability other than the meniscal condition, assign separate evaluations when otherwise warranted under 38 CFR 4.14.
-
Evaluate a noncompensable knee condition by analogy to 38 CFR 4.71a, DC 5257 if there is no associated arthritis the schedular criteria for a noncompensable evaluation under 38 CFR 4.71a, DC 5260 or DC 5261 are not met, and the condition cannot be appropriately evaluated under 38 CFR 4.71a, DC 5258, 5259, 5262, or 5263.
Notes
-
None.